Save £10 or £25 off your first weight loss consultation with code FIRSTWL10 or FIRSTWL25










Thursday 18 June
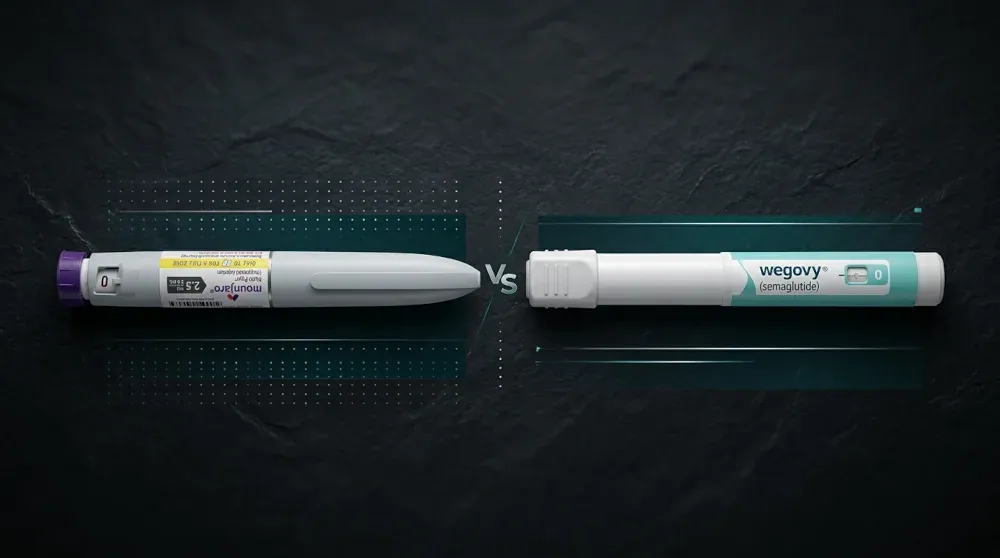
Mounjaro vs Wegovy UK Guide 2025-26
GPhC Pharmacy: 9012581 | Reviewed by: Irfan Mahmud (GPhC: 2080386)
The Only Guide You Actually Need to Read
Two drugs. One goal. Hundreds of questions. The internet is full of articles that look comprehensive but tell you the same four things: tirzepatide targets two receptors, semaglutide targets one, Mounjaro costs a bit more, and crucially, you should 'speak to your doctor.' That's not a guide. That's a disclaimer dressed as content. This article is different. It is drawn from 69 pages of original clinical research, trial analysis, pricing data, and UK-specific regulatory guidance compiled specifically for patients at a GPhC-registered British pharmacy. Every statistic has a source. Every safety note has a mechanism. Every comparison has a caveat. If you read to the end, you will know exactly which drug is right for you, or, at the very least, you will know which questions to take into your consultation rather than walking in blind.
What Is Actually Happening Inside Your Body?
Before comparing drugs, it helps to understand the problem they're solving, because obesity is not a willpower deficit. It is, in large part, a hormonal one. Your gut produces a hormone called GLP-1 (glucagon-like peptide-1) every time you eat. It signals your brain to reduce appetite, tells your pancreas to release insulin, and slows the rate at which food leaves your stomach. In many people living with obesity, this signal is blunted, meaning the brain does not receive adequate fullness cues even when sufficient food has been consumed. The result is a biological drive to eat more, not a character flaw.
"The brain does not receive adequate fullness cues even when sufficient food has been consumed. This is hormonal biology, not a failure of willpower."
Both Mounjaro and Wegovy work by mimicking GLP-1 in pharmacological form, engineered to last days rather than the two minutes your body's natural version survives. A single weekly injection is enough to suppress appetite throughout the week, reduce the frequency and intensity of food cravings, and slow gastric emptying so meals keep you feeling full for significantly longer. The critical difference: Mounjaro (tirzepatide) goes further. It also activates a second receptor GIP (glucose-dependent insulinotropic polypeptide) a mechanism that, when combined with GLP-1 activation, appears to enhance the body's ability to process and oxidise dietary fat. This dual-receptor engagement is not a marketing distinction. It is the fundamental reason why Mounjaro consistently produces greater average weight loss than Wegovy in clinical trials. But here is what almost every comparison article omits: those trials were never designed to compare the two drugs against each other.
Real Results: What the Clinical Trials Actually Show
The most frequently misunderstood aspect of the Mounjaro vs Wegovy comparison is the headline weight loss figures. You will see them everywhere, 22.5% for Mounjaro, 15% for Wegovy. What you rarely see is the context that makes those numbers meaningful. Those figures come from separate trial programmes, SURMOUNT for tirzepatide, STEP for semaglutide, conducted by independent research teams, with different study populations, different follow-up durations, and different background lifestyle interventions. Drawing a straight-line comparison between them is scientifically imprecise. It implies a certainty about relative efficacy that the data does not actually support.
The 2025 STEP UP trial, presented at the American Diabetes Association congress, is the data point that changes the conversation. Wegovy at its newer, higher-dose 7.2 mg HD formulation produced approximately 21% average weight loss over 72 weeks, nearly equivalent to Mounjaro's 22.5% over the same period. The gap that seemed decisive in earlier comparisons is, at matched doses and durations, considerably narrower. What does this mean for the patient standing in front of a pharmacy shelf? It means both drugs are highly effective. It means Mounjaro may produce marginally greater weight loss on average. And it means that for many patients, the decision should turn on other factors entirely, cardiovascular health, contraception use, budget, and NHS eligibility, rather than on a percentage point difference derived from non-comparable trials.
A note on realistic expectations:
The headline figures are trial averages, means across large, diverse populations. Individual response varies significantly based on starting weight, dose reached, dietary adherence, and metabolic profile.
Approximately 10–15% of patients do not achieve meaningful weight loss on GLP-1 class medications, for reasons not yet fully understood. Non-response is not a failure of character, it is a documented pharmacological reality.
Patients with Type 2 diabetes consistently achieve lower average weight loss than non-diabetic populations. Mounjaro at 15 mg produced ~15.7% average loss in T2D patients (SURMOUNT-2) vs ~22.5% in non-diabetic patients (SURMOUNT-1). Set your expectations accordingly.
What to Expect, Week by Week
The most common reason patients abandon weight loss injections prematurely is a mismatch between expectation and reality in the first four weeks. Understanding the treatment arc before you begin is one of the most valuable things this guide can give you.
Weeks 1–4: The Adaptation Phase
The starter doses 2.5 mg for Mounjaro, 0.25 mg for Wegovy are sub-therapeutic by design. They are not intended to suppress your appetite maximally; they are designed to let your gastrointestinal system acclimatise to the mechanism of action. Weight loss at this stage is typically 0.5%–2% of starting body weight. At 100 kg, that is 0.5 to 2 kg. This feels anticlimactic. It is entirely normal. The most important tasks during this phase are tolerability management and habit formation, not weight loss measurement.
Weeks 5–20: Active Titration — When It Starts Working
Monthly dose escalations bring progressively stronger appetite suppression. Most patients report a reduction in what clinicians call 'food noise' the persistent mental preoccupation with eating, cravings, and the next meal that many people with obesity experience as a constant background feature of daily life. Its disappearance is often described as one of the most striking and unexpected effects of both medications. Weight loss rates accelerate to approximately 0.5–1 kg per week for patients who are also adhering to dietary and lifestyle guidance.
Weeks 36–72: Plateau, Maintenance, and the Long Game
By weeks 36–52, most patients will have reached their maintenance dose and achieved a substantial portion of their total weight loss. This is also when the rate decelerates sometimes significantly. A plateau at this stage is not treatment failure. It is a physiological response: as body weight falls, metabolic rate adjusts downward, reducing the calorie deficit that appetite suppression creates. It is documented in both SURMOUNT and STEP trial data. Stopping treatment abruptly is, in most cases, the worst response to a plateau.
⚠ What Happens If You Stop Treatment?
This is the question patients most often avoid asking. The answer is important: weight regain following discontinuation is well documented. In the STEP-4 extension trial, participants who stopped semaglutide after 68 weeks regained approximately two-thirds of their lost weight within a further 48 weeks. This reflects the fact that the hormonal deficit driving appetite dysregulation remains present when medication is removed. Stopping is a clinical decision, not one to make during a plateau or because of a difficult month.
The Real Cost — And How to Think About It
Cost is, in practice, the factor that determines which drug most UK patients choose. Both are long-term treatments. Both escalate in price as doses increase. The gap between them is meaningful over a full treatment course, but it is not the size of gap most comparison articles imply.
Two things are immediately striking from the table above. First: Wegovy is cheaper at the starter dose but catches up and briefly overtakes Mounjaro at mid-titration doses, before both level out at comparable maintenance pricing under the HD formulation. Second: the 72-week total difference is £400–£600, not the dramatic premium many patients assume. The more important budget reality is this: both medications become significantly more expensive than they initially appear because the doses patients begin on are not the doses they maintain. A patient who enters the pharmacy excited by a £99 Wegovy starter dose and a £148 Mounjaro alternative needs to understand that within six months, both will be in the £290–£315 range per month. Plan for maintenance, not for month one.
"Plan for maintenance costs, not for the starter dose. Both drugs cost more than they look from the outside."
NHS Access: Possible, But Not Quick
Both medications are available on the NHS but 'available' requires careful unpacking. Access is gated through specialist tier 3 weight management services, waiting times for which vary from months to years depending on NHS trust and region. NHS Mounjaro is prioritised currently for patients with Type 2 diabetes and BMI ≥ 30. NHS Wegovy is available with BMI ≥ 27 plus a qualifying weight-related condition a lower threshold, but still through specialist referral in most areas (see NICE TA 875). The private prescription route via a GPhC-registered pharmacy offers immediate access, subject to a clinical consultation and eligibility assessment. Some patients begin privately and transition to NHS prescribing once a tier 3 appointment becomes available there is no clinical barrier to doing so, provided the prescribing clinician has a full treatment history.
Side Effects — The Honest Picture
Most side effects from both medications are gastrointestinal nausea, bloating, constipation, diarrhoea and most arise directly from the mechanism of action: the stomach is emptying more slowly than it is accustomed to. This is expected. It is dose-dependent. It peaks at the starter dose and after each escalation step, then eases as the body adjusts. Understanding this in advance prevents the most common treatment error: stopping medication because of side effects that were always going to resolve within a fortnight.
Four Practical Principles That Reduce GI Side Effects Dramatically:
• Eat smaller portions from day one your stomach is now emptying at one-third the previous rate. Attempt your usual portions and you will feel genuinely unwell.
• Choose lower-fat meals during each escalation step. High-fat food slows gastric emptying further on top of the drug's effect. Compounding that mechanism is the most reliable way to guarantee nausea.
• Do not escalate your dose if side effects are still significant. Both titration schedules allow holds at any dose. Escalating out of impatience rather than tolerance leads to avoidable discomfort and early discontinuation.
• Sip fluids throughout the day rather than drinking large volumes at once. Hydration is critical, but gulping aggravates nausea. Aim for 1.5–2 litres spread across the day.
Where the Two Drugs Differ on Side Effects
Mounjaro's additional GIP mechanism brings some side effects that are absent or less common with Wegovy. A small proportion of Mounjaro users experience a resting heart rate increase of 5–15 beats per minute generally not clinically significant in healthy patients, but warranting monitoring in those with pre-existing cardiac conditions. Injection site reactions, including redness and mild swelling at the injection point, are also reported at a slightly higher frequency with tirzepatide. Wegovy users report marginally higher rates of headache, fatigue in the early weeks, and gallstone formation the latter being a documented risk of rapid weight loss through any mechanism, not specific to semaglutide. The most serious side effects for both medications acute pancreatitis, severe hypersensitivity reactions, intestinal obstruction are rare. They are not hypothetical, and patients should be aware of their symptoms. But they should not dominate the decision for patients without pre-existing risk factors. The risks of undertreated obesity cardiovascular disease, Type 2 diabetes, joint damage, cancer are not rare.
Four Differences That Actually Matter
1. Oral Contraception — A Safety Note That Is Missing From Most Guides
Mounjaro's slowing of gastric emptying can reduce the absorption of oral contraceptive pills. The pill relies on timely intestinal absorption to maintain efficacy; when gastric transit is delayed, that absorption is compromised. The MHRA recommends that patients starting Mounjaro and at each dose escalation use additional barrier contraception for at least four weeks. This is not about compliance history. It is pharmacokinetics. For patients who rely on the combined or progestogen-only pill and prefer not to use additional contraception, Wegovy is the clinically safer choice. This interaction has not been established to the same degree with semaglutide.
2. Cardiovascular Benefit — The SELECT Trial
Wegovy is the only weight loss injection currently holding an MHRA-approved cardiovascular indication. The SELECT trial over 17,500 participants, 33.5 months of follow-up showed that semaglutide 2.4 mg reduced the risk of major adverse cardiovascular events (heart attack, stroke, cardiovascular death) by 20% compared to placebo in adults with established cardiovascular disease. This benefit was observed independently of weight loss achieved, suggesting a cardiovascular effect beyond appetite suppression alone. Mounjaro does not currently hold this indication. The SURPASS-CVOT trial showed cardiovascular non-inferiority to dulaglutide, and Eli Lilly has indicated plans to seek MHRA approval for a cardiovascular indication but as of mid-2026, that approval has not been confirmed. If you have a history of heart attack, stroke, or significant cardiovascular disease: Wegovy is currently the clinically preferred first choice.
3. Type 2 Diabetes — The Case for Mounjaro
If you have Type 2 diabetes alongside obesity, Mounjaro's dual GIP/GLP-1 mechanism offers a genuinely differentiated benefit: addressing glycaemic control and weight simultaneously through two distinct pathways. It is also the medication prioritised under current NHS specialist commissioning for this population, giving T2D patients the most realistic NHS access pathway in 2026. For patients without diabetes, this distinction largely disappears.
4. Is Oral Wegovy Available in the UK? (The Answer That Keeps Being Misunderstood)
⚠ No. Oral semaglutide for weight management is not MHRA-licensed in the UK.
A once-daily oral semaglutide tablet was approved by the FDA in the US in 2024 and has generated significant discussion in UK online communities including r/UKMounjaro and r/UKWeightLoss. This has created a widespread incorrect impression that the same product is available to UK patients. It is not. UK oral semaglutide (Rybelsus) exists only in lower doses approved for Type 2 diabetes management it is not approved for weight loss. Any supplier offering 'oral Wegovy' to UK patients is operating outside the current MHRA licence.
How to Choose: The Framework
The honest conclusion of this entire guide, distilled:
TABLE
"The medication that you can access, afford, and tolerate is the right one for you. The goal is to start, and to maintain."
Neither Mounjaro nor Wegovy is categorically superior for all patients in all circumstances. The trial data is compelling for both. The differences that exist are real but they are nuanced, and they apply to specific patient subgroups rather than to the general population. What this means in practice: if you have established cardiovascular disease, Wegovy is the evidence-based first choice. If you have Type 2 diabetes, Mounjaro earns its premium. If you take the oral contraceptive pill, Wegovy removes one complication. In every other scenario including the vast majority of patients who have none of these differentiating factors your decision can legitimately turn on cost, availability, and what your prescriber has direct experience managing. Both drugs will work. The evidence is not in question. What determines your outcome is not which injection you choose it is whether you start, whether you stay on it, and whether you use the appetite suppression it creates to build dietary and lifestyle habits that can outlast the medication itself.
About This Guide
This article was produced under the clinical supervision of Irfan Mahmud, Superintendent Pharmacist, GPhC Registration: 2080386.
Dispensed and reviewed by our GPhC-registered pharmacy, Registration: 9012581, regulated by the General Pharmaceutical Council (pharmacyregulation.org).
All treatments discussed are prescription-only medicines (POM). This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional before starting, stopping, or changing any medication.
Report suspected side effects via the MHRA Yellow Card scheme: yellowcard.mhra.gov.uk
Sources: Jastreboff AM et al. SURMOUNT-1. NEJM 2022. | Wilding JPH et al. STEP-1. NEJM 2021. | Wharton S et al. STEP UP. ADA 2025. | Lincoff AM et al. SELECT trial. NEJM 2023. | Bhatt DL et al. SURPASS-CVOT. NEJM 2025. | MHRA SmPCs — Mounjaro and Wegovy, updated 2024. | NICE TA875. | NHS England Commissioning Guidance 2024.